In recent newsletters, I have offered some warnings against certain science-related ideas that show up in the news—ideas used to corral large swaths of the population into agreement about various topics. One of these is “scientific consensus,” others being “misinformation” or that we should “trust the science.” These relatively new concepts are almost universally used to discourage people from entertaining or investigating ideas or information that make people with authority uncomfortable.
Another widely used method for accomplishing something very similar is even more insidious, and it hides behind some of the most egregiously manipulative “science” presented to the public. I’m talking about the use of mathematical models.
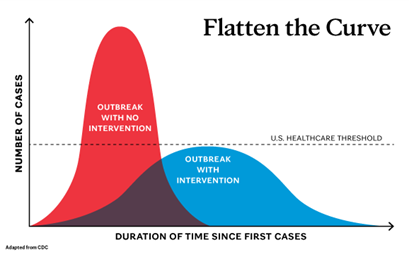
“Three Weeks to Flatten the Curve”
Maybe you recall, in the very early days of the COVID-19 phenomenon, there was an idea that flooded the public space: “three weeks to flatten the curve.” That idea was the invention of Dr. Neil Ferguson of Royal College London. Based on a mathematical model he had developed and promoted to governments around the world, he proposed that with three weeks of everyone staying home and avoiding public interaction, the number of COVID-19 cases could be dramatically reduced. This, in turn, would prevent hospitals from being overrun with patients sick with COVID-19. Various versions of this image were ubiquitous in the media at the time.
As we all know, those three weeks turned into months and, for many schools such as my daughter’s, over a year of stay-at-home orders. Even Dr. Ferguson himself admitted at the end of 2021 that his model might not have been quite right, that he might have “oversimplified” things. But by that point, the model had already served its purpose, which was to manipulate the public into accepting and even advocating lockdowns for an extended period of time.
What Are Mathematical Models Used For?
Mathematical models in medicine are tools commonly used for at least two purposes. One is to predict possible future outcomes (for diseases, for the climate, for world population, etc.) based upon various assumptions. Given those assumptions, the model is charged with predicting how that outcome would change if, say, people adopt some new set of behaviors (people isolating, for example).
Another use is to estimate a different outcome in the past if various things had been different. For example, what if more people did or didn’t get an mRNA shot?
For every mathematical model to make a prediction, some initial assumptions have to be fed into it. Regarding the model predicting how much COVID-19 would overwhelm hospitals, these initial assumptions included things like how contagious and how infectious the virus was, how many infected people would develop the illness, how many of those would need to be hospitalized, how many hospitalized would need critical care, and perhaps most importantly, how effective social isolation would be in reducing the spread, and more.

It is key to understand that none of these were known at the time. Dr. Ferguson made up values for each of these based on what he considered best guesses, he plugged them into his model, then let the mathematics in his model generate predictions based on those initial assumptions. Since it was a mathematical model, it had all the legitimacy that scientific findings claim, and he sold the world on his results.
Note the pattern happening here. Based upon a large set of chosen assumptions, the model can be designed to predict a dire outcome if people don’t adopt a prescribed behavior. In fact, models can make any prediction you want, simply by changing the assumptions built into it.
Models and Public Policy
I won’t go into the wide range of negative health consequences of the global lockdowns that have now been documented. My point is that it was a single model that stoked the fear that drove the policy globally, and even the model’s author later said, “Oops, I might have overestimated some things.”
Mathematical Models and “Lives Saved” Claims
Another example of psychological manipulation through mathematical models is exemplified in a study published in 2025 claiming that “COVID-19 vaccinations averted 2.5 million deaths during 2020-2024.” Whenever you see a headline stating lives saved by vaccinations, you should always ask, How do they know?
No one can possibly know how many lives would have been lost had the people who got the mRNA shot not gotten the mRNA shot. How is the estimated number of deaths averted generated? A mathematical model, of course. And what gets fed into the model for it to spit out a number like that? Assumptions.
It is important to keep in mind that the medical community pushed mRNA vaccinations with an unparalleled sense of urgency and even existential panic. As a consequence, that same community has a strong vested interest in having the vaccinated public believe that it made the right decision.
The estimates of lives saved by the shots start with a big load of loaded assumptions that get fed into the model, not the least of which are the two that directly determine the very thing the model is trying to estimate: the fatality rate caused by infection, and how effective the vaccine is at preventing deaths in those who get infected. If you don’t feed the model with information about how effectively the shots prevent death, then the model can’t tell you anything about lives saved.
Clearly, the higher you turn the dial on the estimated effectiveness of the vaccine, and the higher you turn the dial on how many infected people die, you will find a correspondingly higher estimated number of people who didn’t die if they got the shot but would have died without it.
How Assumptions Shape Results
To get a sense of the difference it makes to use different assumptions within your model, a previous study published in 2022 estimated that the shots had prevented a whopping 19.8 million deaths globally just between Dec 2020 and Dec 2021. How could the shots have possibly been so fantastically protective? Easy, just assume a high number of people infected will die, and assume that the vaccination is 95% effective at preventing infection. Neither was true, but these assumptions fed into the model are never part of the news story about the reported finding.
Note that billions of additional people received shots between the endpoint of the estimate in the 2022 study referenced above and the 2025 study referenced above. The question that needs asking is this: if the shots in fact worked to prevent deaths as well as the 2022 study concluded, why were fewer lives saved by the shots by the end of 2024 (the total estimated at 2.5 million) even though billions more people around the globe got shots after the end of the 2022 study?

Also, there is the glaring omission in deaths-averted studies like these. Namely, deaths caused by the shots. Here’s a case in point: two separate studies – one out of Italy and one from South Korea – looked at medical records of many millions of mRNA-shot people and actually counted (as opposed to modeled) the number of cancer diagnoses above the historical baseline in each country. The findings are shocking and ominous.
Cancer Risks in Italy and South Korea
Italy:
A 23% increased risk of being diagnosed with cancer within 1 year after 1 or more mRNA doses among people who were vaccinated but had not had a prior COVID-19 infection.
All dots right of the vertical dotted red line represent an increased cancer risk. Red dots denote statistically significant increased risk.
South Korea:
At 1 year after vaccination, overall risk of cancer was 27% higher among the vaccinated. The risk of particular cancers was exceptionally high. Prostate cancer carried a 69% higher risk, while lung cancer had a 53% higher risk. Note that this study involved over 8 million people, so there is no discounting the findings as a fluke.
A third peer-reviewed study out of Japan looked in the tumor tissue of a woman with a highly aggressive breast cancer. Finding? Spike protein was highly expressed within the tumor tissue, driving cellular replication. From the paper:
“[I]t might be possible that the administered mRNA was retained in cancer cells leading to more aggressive nature, or any contaminated template DNA, other contaminated oncogenic DNA, or reverse-transcribed DNA that codes the spike protein, might be integrated into the host genome to confer increased malignancy. This possibility would be relevant to intrinsic expression of spike protein in cancer cells.”
I have been co-author on not one, not two, not three, but four papers explaining why these shots could lead to more overall and more aggressive cancers. Again, we had no crystal ball when researching and writing these papers. It was all there for anyone paying attention to see.
The Benefit/Risk Equation
Increased cancer following mRNA shots is just one outcome that could trim some of those saved lives off of the 2.5 million averted deaths the model estimated. Add to this the increase in myocarditis, Parkinson’s, heart disease, fatal bacterial infections, and even a 37% general excess mortality, and the benefit/risk equation becomes more nebulous. Dial down the optimistic assumption of vaccine efficacy, then take into account the virtually zero infection fatality rate for those under 50, and the few millions of lives saved evaporate into modeling air.
Are Models Inherently Bad?
Models are not inherently deceptive. Weather forecasting continuously relies upon models, as do stock market predictions, finances, utilities, real estate, and many other fields. Models allow for predictions. Models run on initial assumptions. The accuracy of the model’s predictions is directly proportional to the validity of the starting assumptions.
But always keep in mind that models require an input of assumptions. If there is a vested interest in what the modelers want you to believe and act on, feeding in skewed assumptions can make the model predict a future as dire as necessary to compel behavior.
Wrapping Up: What Can You Do?
I’m not putting this information out there to be a downer for those who chose to or who were coerced into getting an mRNA shot. Even the un-shot are likely exposed via exosomes, aka ‘shedding.’ We’re all in this together. The light at the end of this tunnel is that there are steps anyone can take to minimize the risk of that exposure.
Remember, the two rules for a healthy life: risk management and damage control. I can give you my best-evidence-based recommendations for how to optimize cancer prevention, degrade spike proteins, and amp up your innate immunity to prevent future infections.
If you made it this far, reward yourself with a whopping 0% off your next scheduled consultation. But don’t tell anybody. This is your personal bonus for your perseverance. It takes time to put articles like this together so I appreciate your commitment to reading it through.
Schedule via phone at 503-719-4806, email to drnigh_info@gregnigh.com, or via gregnigh.com/Schedule.